Billing rules for inpatient and outpatient providers are complicated, and as a result, providers' small habitual practices can have major financial implications. Accurate billing depends on accurate documentation of HPI, family history, social history, among others. Some of these can be enforced using templates, but when it comes to the assessment and plan, much of the importance is in the wording of documentation (especially in hospital billing) and the assessment of the complexity (especially in profession billing). Here, I describe some of my investigations in this area.
Many times, however, the comorbid condition exists but the final billing fails to reflect their existence. I conducted a contextual inquiry to learn about documentation pitfalls that can affect providers and classified them into 6 types of errors:
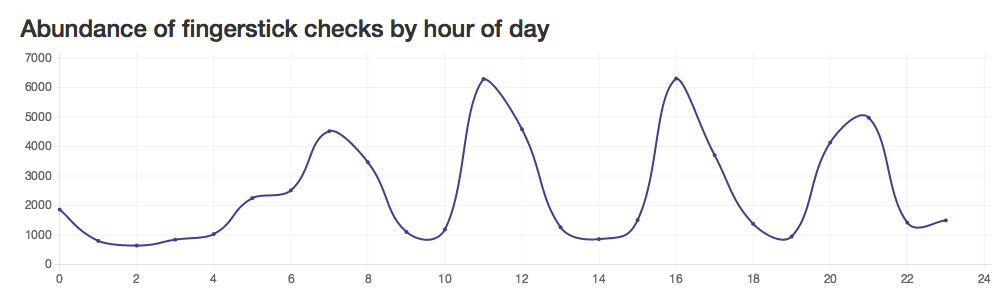
One type of professional billing is based on the complexity of medical decision making, and has a number of rules that can be difficult to remember. I ran analytics on these data to find deficits or outliers in billing.


Using these types of analyses, providers can see if they are outliers in choosing level of service. Further work will help providers see financial magnitude of these outliers.
Probably the biggest intervention has been to help providers quickly calculate billing level and see their gaps in documentation. I created a tool to help calculate the medical complexity, which providers can use on their phones before closing notes.
Update:
People started asking for this calculator, so I decided to make it available on the Apple App Store. Enjoy! Get BillUp on the Apple App Store

Inpatient Hospital Billing (DRGs)
Provider documentation helps classify patients into a DRG (Diagnosis-related group) and various risk-stratifying scores. The DRGs a patient falls into, and whether or not there is enough documentation to support the existence of a comorbid condition (CC) or major comorbid condition (MCC), can have significant financial implications (see table).2017 DRG medicare reimbursements for our hospital
MS Diagnosis-related group (DRG)
|
W/O CC
|
W/ CC
|
W/ MCC
|
SPINAL DISORDERS & INJURIES
|
$8,024.21
|
$14,790.38
|
|
NERVOUS SYSTEM NEOPLASMS
|
$9,585.56
|
$12,425.49
|
|
DEGENERATIVE NERVOUS SYSTEM DISORDERS
|
$10,450.70
|
$17,278.46
|
|
MULTIPLE SCLEROSIS & CEREBELLAR ATAXIA
|
$7,600.51
|
$9,803.01
|
$15,731.11
|
ACUTE ISCHEMIC STROKE W USE OF
THROMBOLYTIC AGENT
|
$14,711.98
|
$17,606.97
|
$25,540.65
|
INTRACRANIAL HEMORRHAGE OR CEREBRAL
INFARCTION
|
$6,965.89
|
$9,734.88 (OR TPA within 24hr
pre-arrival)
|
$16,348.93
|
NONSPECIFIC CVA & PRECEREBRAL
OCCLUSION W/O INFARCT
|
$8,080.21
|
$12,481.48
|
|
TRANSIENT ISCHEMIA
|
$6,880.96
|
||
NONSPECIFIC CEREBROVASCULAR DISORDERS
|
$6,863.23
|
$9,155.33
|
$15,197.28
|
CRANIAL & PERIPHERAL NERVE
DISORDERS
|
$8,576.70
|
$12,315.36
|
|
VIRAL MENINGITIS
|
$8,955.61
|
$15,837.50
|
|
HYPERTENSIVE ENCEPHALOPATHY
|
$6,545.92
|
$8,838.95
|
$14,705.45
|
NONTRAUMATIC STUPOR & COMA
|
$7,144.14
|
$11,727.40
|
|
TRAUMATIC STUPOR & COMA, COMA >1
HR
|
$8,643.90
|
$11,961.65
|
$18,739.02
|
TRAUMATIC STUPOR & COMA, COMA <1
HR
|
$7,531.45
|
$10,652.28
|
$18,696.09
|
CONCUSSION
|
$7,127.34
|
$9,482.90
|
$13,850.58
|
OTHER DISORDERS OF NERVOUS SYSTEM
|
$6,592.58
|
$8,586.97
|
$14,711.98
|
BACTERIAL & TUBERCULOUS INFECTIONS
OF NERVOUS SYSTEM
|
$19,988.66
|
$22,212.63
|
$32,496.28
|
NON-BACTERIAL INFECT OF NERVOUS SYS EXC
VIRAL MENINGITIS
|
$11,913.12
|
$16,929.42
|
$28,967.60
|
SEIZURES
|
$7,456.78
|
$14,871.57
|
|
HEADACHES
|
$6,910.82
|
$9,939.27
|
Many times, however, the comorbid condition exists but the final billing fails to reflect their existence. I conducted a contextual inquiry to learn about documentation pitfalls that can affect providers and classified them into 6 types of errors:
- Poor specificity
- Omission (things with objective indicators elsewhere)
- Omission (things subjective)
- Technical or linguistic
- Timing
- Conflicting information
Errors of Poor Specificity
Vague problems are typically billed lower than specific ones, etiologies
Examples
- heart failure is ambiguous -> instead, specify systolic/diastolic heart failure
- respiratory failure or dyspnea is ambiguous -> instead specify respiratory failure secondary to community acquired pneumonia
- Encephalopathy is ambiguous -> instead specify etiology
- chest pain is ambiguous
Errors of omission
When imaging or labs are abnormal but the documentation does not address the diagnosis and plan. Hospital cannot bill on the basis of lab or imaging report or pathology report alone.
Examples
- Cerebral edema - midline shift mentioned in imaging but not in assessment/plan
- Brain compression
- Moderate/Severe protein/calorie malnutrition – this is a CC/MCC (Comorbid condition), always mentioned in the nutrition note, but hospital cannot bill based on a nutrition note is note enough
- Morbid obesity – this is a CC/MCC
- Anemia, thrombocytopenia, hypokalemia – abnormalities in CBC/BMP contribute to diagnoses and CC/MCC, but are often ignored by providers
Professional Billing


Using these types of analyses, providers can see if they are outliers in choosing level of service. Further work will help providers see financial magnitude of these outliers.
Probably the biggest intervention has been to help providers quickly calculate billing level and see their gaps in documentation. I created a tool to help calculate the medical complexity, which providers can use on their phones before closing notes.
Update:
People started asking for this calculator, so I decided to make it available on the Apple App Store. Enjoy! Get BillUp on the Apple App Store